How Tirzepatide Works

How Tirzepatide Works:
Here is the canned answer that doctors have learned from their pharmaceutical reps and that pharma companies are comfortable releasing and explaining- less stomach acid, slower food clearance = prolonged satiety, or feeling fuller longer. But let’s dive into some real science behind it.
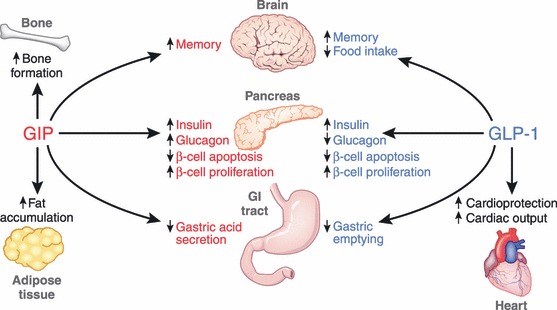
Tirzepatide is a twincretin, fancy talk for two incretins working together. It is a GIP, gastric inhibitory peptide and GLP-1, glucagon-like peptide, combination therapy. These two pathways have some similar actions in common, but differ in other important ways. Incretins are metabolic hormones that are released in response to food intake. They decrease blood glucose levels by stimulating insulin release from pancreatic beta cell islets. Clearing superfluous glucose has some pretty unique anti inflammatory implications that apply to pre diabetics and people battling stubborn obesity. On a more physical function note, GIP reduces the amount of stomach acid produced and GLP-1 slows the rate of gastric emptying. This tandem of activity keeps the user feeling fuller more quickly and for longer. The ensuing, prolonged gastric distention keeps ghrelin levels lower. Ghrelin is a hunger inducing hormone that is released when the stomach is empty. The vagus nerve, whose end processes lie in grehlin producing areas, then carries the “ I am empty” message to the brain to stimulate a plan to find the next meal. It's a complex dance with factors like dopamine 2 receptor, D2R, expression in the hypothalamus to dictate feeding behavior. Quick digression here, but D2R expression is the missing element in brain scans of addicts as seen below.

The lack of D2R expression creates an anhedonic feeling that drives the pursuit of compensatory things like high fat and sugary food sources. Keeping ghrelin low via GIP/GLP-1 agonism blunts the anticipatory dopamine response to food, lowering intake in the process. In particular, GLP-1 agonists lower rates of phasic dopamine blasts in the nucleus accumbens core. The nucleus accumbens is the hub for classic addiction driven behaviors like reward anticipation and seeking behaviors. With dopamine hyper responses to food blunted by GLP-1, traditional cues like stress don’t wield the same power to induce overconsumption. Next, GIP and GLP-1 facilitate better memory by enhancing neuronal progenitors and augmenting long term potentiation. One theory here is that such improved pathways can rewire the brain to think about food differently even after cessation of treatment. I will debunk that here as wishful thinking. After much feedback from my clients, it is clear that appetite returns to original levels shortly after stopping treatment. Does that mean you will have to take it forever? The short answer is no and maybe. Like with any addiction, positive lifestyle changes while on treatment must be practiced and locked in as habitual behavior. Gaining all of your weight back is simply a relapse to addiction. I do have several successful clients, who once at goal, now cruise with a light maintenance dose. Obesity is a condition often driven by insurmountable predispositions. Much like genetically imposed high blood pressure or cholesterol, an obese condition may require consistent medication. Back to the science, Endogenous GIP and GLP-1 both control food intake and satiety by hypothalamic receptor interactions. So, it's a lot more than making you sick if you eat too much. The punishment approach was tried and failed in alcoholics with the drug Antabuse (disulfiram). Alcoholics simply quit taking it or drank through the side effects. Instead, the twincretin mechanism of GIP/GLP-1 agonism helps set you up for success before you take the first bite. I didn't touch on the buzz of leptin (satiety hormone) resistance due to its inverse relationship with ghrelin covered above.
Some final thoughts:
GIP is not the perfect partner for GLP-1 in my opinion due to its lipogenesis induction and promotion of fat accumulation. I assume this is why retatrutide is adding glucagon agonism to offset some of these actions. However, the combo works and the end seems to justify the means. Some things to avoid for optimal results include marijuana, high stress, steroids and other actions that directly increase ghrelin and cortisol. Cortisol increases ghrelin. Some safe supplementation to consider would be intranasal oxytocin and ashwaganda. Ashwaganda lowers cortisol, so in turn grehlin and gives a slight testosterone boost. Oxytocin, my favorite peptide by the way, lowers ghrelin and cortisol, prevents muscle wasting, decreases fat cell size, helps ensure proper D2R expression and is an awesome anti-inflammatory for all things brain! Lastly, create a skinny microbiome. The cheapest, easiest hack is Lifeway Kefir (awesome functional microbiota) and fiber, especially in the evening. Try to limit or avoid simple sugars after lunch. Done for now, that's another article completely.
Summary Chart:
References:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4020673/
https://mappingignorance.org/2017/08/21/child-obesity-brain-function/obesity-brain-scan/